|
|
|||||||||
|
|||||||||

 |
Dr N Arber |
Colorectal cancer (CRC) is a major health concern. It is anticipated that more than 1 million new cases will be identified worldwide this year. Colorectal cancer is the second leading cause of cancer death, with a 50% mortality rate. However, colorectal cancer is preventable by early detection of pre-malignant lesions in average-risk populations, chemoprevention for high-risk populations, and lifestyle modifications.
Chemoprevention
Chemoprevention has emerged as a science during the past decade. Chemoprevention is defined as the use of specific natural or synthetic agents to reverse, suppress, or prevent the carcinogenic process from progressing to invasive carcinoma. The ideal chemopreventive agent should be taken orally, once daily or weekly, with no side effects, and be efficacious and cheap. There are many chemopreventive agents with proven efficacy and some dietary substances have potential chemopreventive properties
(Table 1). However, all of these agents only have a marginal effect. The most promising agents for chemoprevention are the non-steroidal anti-inflammatory drugs (NSAIDs).1
Table 1. Proven chemopreventive agents and dietary substances with potential chemopreventive properties.
| Proven chemopreventive agents | Dietary substances |
|
Hormone replacement therapy |
Green and black tea polyphenols |
Non-steroidal Anti-inflammatory Drugs for Chemoprevention
More than 1 million people worldwide take NSAIDs. More than 70 million prescriptions and 30 million over-the-counter sales were recorded in the USA in 1998. The association between NSAID consumption and colorectal cancer was accidentally found. Dr Waddell first noticed that some of the members of his family with familial polyposis experienced regression of the polyps when consuming NSAIDs for a variety of reasons unrelated to familial polyposis. Following this anecdotal finding, studies were performed in animal models. Kudo et al found that rats coadministered indomethacin and a colon carcinogen developed fewer tumours.2 Following this primary research, more than 100 well-conducted studies have demonstrated that aspirin and NSAIDs prevent colorectal carcinoma
(Table 2).
Table 2. Prevention of colorectal cancer by aspirin or non-steroidal anti-inflammatory drugs.
|
Reduction in incidence (% of animals with tumours) |
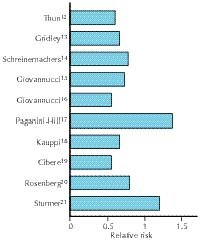
Nine retrospective studies clearly demonstrated the protective effects of NSAIDs. The relative risk of colon cancer was approximately 50% for people taking NSAIDs compared with non-users (Figure 1).3-11 Eight of 10 prospective studies demonstrated the same phenomenon (Figure 2).12-21 NSAIDs can also prevent adenoma formation. Overall, the protective effects of NSAIDs were shown in 23 of 25 clinical studies strong evidence for this phenomenon.
Figure 1. Summary of retrospective studies of non-steroidal anti-inflammatory drug use and colorectal cancer.
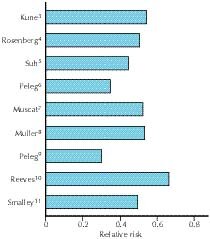
Figure 2. Summary of prospective studies of non-steroidal anti-inflammatory drug use and colorectal cancer.
Molecular Pathways of Action
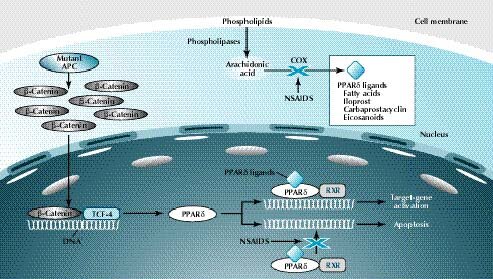
There are 2 pathways that may be relevant to efficacy of NSAIDs in preventing colorectal cancer (Figure 3). NSAIDs inhibit the cyclooxygenase (COX) enzyme. By inhibiting the COX enzyme, formation of prostaglandin is prevented and proliferation is inhibited. It has recently been found that NSAIDs also inhibit the APC ![]() -catenin pathway by inhibiting proliferator peroxisome-activating receptors. In this way, they complement the process of apoptosis. Therefore, NSAIDs both inhibit proliferation and augment apoptosis.
-catenin pathway by inhibiting proliferator peroxisome-activating receptors. In this way, they complement the process of apoptosis. Therefore, NSAIDs both inhibit proliferation and augment apoptosis.
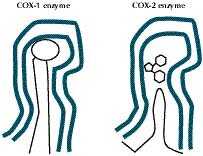
However, NSAIDs are toxic substances that may cause gastrointestinal bleeding. There are 2 COX enzymes COX-1 and COX-2 (Figure 4). COX-1 is a 'housekeeping' gene, which protects the gastrointestinal mucosa and is constantly expressed. The COX-2 enzyme is inducible and is not found in normal appearing mucosa. However, it is induced as a consequence of inflammation or carcinogenetic stimuli.
Figure 3. Molecular biological pathways of non-steroidal anti-inflammatory drugs.
Cyclooxygenase-2 Inhibitors
The COX-1 and COX-2 enzymes are similar, with approximately 60 to 70% homology. However, the COX-2 enzyme has a wider channel and a side pocket that contains the binding site of the specific COX-2 inhibitor (Figure 4).
Figure 4. Structural differences of cyclooxygenase-1 and cyclooxygenase-2 enzymes.
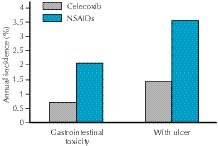
Currently, there are 2 main COX-2 specific inhibitors available celecoxib and rofecoxib. These 2 agents are similar, with a comparative side effect profile, which is significantly better than that of standard NSAIDs. In the Celecoxib Long-term Arthritis Safety Study (CLASS), in which more than 8000 patients with rheumatoid or osteoarthritis were recruited in 386 sites, celecoxib was associated with a lower incidence of symptomatic ulcers and ulcer complications than NSAIDs.22 Celecoxib was associated with less chronic gastrointestinal blood loss, gastrointestinal intolerance, and renal or liver toxicity than NSAIDs (Figure 5). Low toxicity at high doses suggests that celecoxib may be appropriate for long-term preventive therapy.
Figure 5. Gastrointestinal toxicity with celecoxib and non-steroidal anti-inflammatory drugs (NSAIDs).
While there has been debate about the cardiovascular safety of these agents, data from the Celecoxib Cardiovascular Safety Database indicate that celecoxib is safe. Results from several trials involving more than 37,000 patients indicate that the cardiovascular safety profile of celecoxib equalled that of NSAIDs.
Celecoxib for Prevention of Colorectal Cancer
Evaluation of the effect of celecoxib on a variety of cell lines, including normal cells from rat ileum as controls and the same cell lines transected with the oncogenes RAS and bcl2 and anti-sense bak, showed that celecoxib inhibited the malignant cells significantly more than the normal cells.23 In an animal model of colon cancer, rats were injected with a carcinogen. After 52 weeks, 90% of rats receiving the placebo developed tumours compared with only 10% of the animals receiving celecoxib, clearly demonstrating the potential of celecoxib to prevent cancer. In addition, the tumour volume was significantly decreased among rats receiving celecoxib compared with control rats.
In a landmark study by Oshima et al24 involving mice with mutations in the APC genes, untreated mice produced 652 tumours per animal. When one COX-2 copy was disabled, the mice produced only 224 tumours per animal and when both copies were disabled, there were only 93 tumours per animal, clearly demonstrating the importance of COX-2 in colorectal carcinogenesis.
Immunohistochemistry shows that normal mucosa in the colon does not express COX-2. However, COX-2 is overexpressed in colorectal carcinogenesis as shown by its presence in polyps, primary cancers, and metastases. Steinbach et al studied the effects of COX-2 selective inhibition on colorectal adenomas in patients with familial adenomatous polyposis in a placebo-controlled, double-blind trial.25 Seventeen patients received placebo, while 32 received celecoxib 100 mg or 400 mg twice daily for 6 months. Patients receiving celecoxib 400 mg did significantly better than those receiving placebo, experiencing a 30% reduction in the number of colorectal polyps. There was also a significant change in the area of duodenal plaque-like polyps.
Celecoxib is effective for cancer prevention in people with familial polyposis, although less is known about its role in sporadic polyps. Three international multicentre studies have been launched during the past 2 years to evaluate the efficacy of the new COX-2 specific inhibitors in preventing the recurrence of sporadic colorectal polyps, and to find the best drug and dosage. Each study was designed to recruit between 1500 and 2000 patients from more than 100 sites during a 3-year period. Enrolment to all the studies has recently been completed. The primary endpoint in all 3 studies is the number of patients with adenomas. Celebrex is being evaluated in 2 studies. The first one is a joint venture of Pharmacia and the National Cancer Institute (NCI) and was launched in December 1999. The second celebrex trial is sponsored solely by Pharmacia, and was launched in March 2001. Rofecoxib is being evaluated in another study that was launched in April 2000, and is being run by Merck Sharp and Dohm. The 3 trials are ongoing to determine whether COX-2 inhibitors can prevent adenoma formation in this group of patients. The first study was launched in December 1999 by the NCI to compare celecoxib 200 mg and 400 mg twice daily with placebo. The second study, launched in April 2000, will compare rofecoxib 25 mg with placebo. The third study will compare celecoxib 400 mg with placebo.
Why Celecoxib?
From both an objective and subjective point of view, based on evidence and his own experience, Dr Arber recommended the use of celecoxib for chemoprevention for patients with familial adenomatous polyposis. This recommendation is based on cell culture data and published animal studies, while the proof of the concept has been shown in the clinical trial by Steinbach et al.25 Celecoxib is currently the only drug that is approved by the USA Food and Drug Administration for the treatment of familial adenomatous polyposis.
The Future
Interestingly, COX-2 is markedly upregulated in a number of other cancers, including lung, breast, prostate, ovarian, pancreatic, and cholangiocarcinoma. Inhibition of overexpression of COX-2 appears to be most promising for breast cancer and chemoprevention by celecoxib or ibuprofen has been shown in rats with breast tumours.
References
1. Oviedo JA, Wolfe MM. Clinical potential of cyclo-oxygenase-2 inhibitors. Bio Drugs 2001;15:563-572.
2. Narisawa T, Sato M, Tani M, Kudo T, Takahashi T, Goto A. Inhibition of development of methylnitrosourea-induced rat colon tumors by indomethacin treatment. Cancer Res 1981;41: 1954-1957.
3. Kune GA, Kune S, Watson LF. Colorectal cancer risk, chronic illnesses, operations, and medications: case control results from the Melbourne Colorectal Cancer Study. Cancer Res 1988;48: 4399-4404.
4. Rosenberg L, Palmer JR, Zauber AG, et al. A hypothesis: nonsteroidal anti-inflammatory drugs reduce the incidence of large-bowel cancer. J Natl Cancer Inst 1991;83:355-858.
5. Suh O, Mettlin C, Petrelli NJ. Aspirin use, cancer, and polyps of the large bowel. Cancer 1993;72:1171-1177.
6. Peleg II, Maibach HT, Brown SH, Wilcox CM. Aspirin and non-steroidal anti-inflammatory drug use and the risk of subsequent colorectal cancer. Arch Intern Med 1994;154:394-399.
7. Muscat JE, Stellman SD, Wynder EL. Nonsteroidal antiinflam-matory drugs and colorectal cancer. Cancer 1994;74:1847-1854.
8. Muller A, Hurlimann R, Meyenberger C, Staub P, Kobler E, Ammann R. Sulindac in familial adenomatous polyposis coli preliminary findings of a prospective study [article in German]. Schweiz Med Wochenschr 1994;124:651-654.
9. Peleg II, Lubin MF, Cotsonis GA, Clark WS, Wilcox CM. Long-term use of nonsteroidal antiinflammatory drugs and other chemopreventors and risk of subsequent colorectal neoplasia. Dig Dis Sci 1996;41:1319-1326.
10. Reeves MJ, Newcomb PA, Trentham-Dietz A, Storer BE, Remington PL. Nonsteroidal anti-inflammatory drug use and protection against colorectal cancer in women. Cancer Epidemiol Biomarkers Prev 1996;5:955-960.
11. Smalley W, Ray WA, Daugherty J, Griffin MR. Use of nonsteroidal anti-inflammatory drugs and incidence of colorectal cancer: a population-based study. Arch Intern Med 1999;159:161-166.
12. Thun MJ, Namboodiri MM, Heath CW Jr. Aspirin use and reduced risk of fatal colon cancer. N Engl J Med 1991;325: 1593-1596.
13. Gridley G, McLaughlin JK, Ekbom A, et al. Incidence of cancer among patients with rheumatoid arthritis. J Natl Cancer Inst 1993;85:307-311.
14. Schreinemachers DM, Everson RB. Aspirin use and lung, colon, and breast cancer incidence in a prospective study. Epidemiology 1994;5:138-146.
15. Giovannucci E, Rimm EB, Stampfer MJ, Colditz GA, Ascherio A, Willett WC. Aspirin use and the risk for colorectal cancer and adenoma in male health professionals. Ann Intern Med 1994; 121:241-246.
16. Giovannucci E, Egan KM, Hunter DJ, et al. Aspirin and the risk of colorectal cancer in women. N Engl J Med 1995;333:609-614.
17. Paganini-Hill A. Aspirin and colorectal cancer: the Leisure World cohort revisited. Prev Med 1995;24:113-115.
18. Kauppi M, Pukkala E, Isomaki H. Low incidence of colorectal cancer in patients with rheumatoid arthritis. Clin Exp Rheumatol 1996;14:551-553.
19. Cibere J, Sibley J, Haga M. Rheumatoid arthritis and the risk of malignancy. Arthritis Rheum 1997;40:1580-1586.
20. Rosenberg L, Louik C, Shapiro S. Nonsteroidal antiinflammatory drug use and reduced risk of large bowel carcinoma. Cancer 1998;82:2326-2333.
21. Sturmer T, Glynn RJ, Lee IM, Manson JE, Buring JE, Hennekens CH. Aspirin use and colorectal cancer: post-trial follow-up data from the Physicians' Health Study. Ann Intern Med 1998;128: 713-720.
22. Silverstein FE, Faich G, Goldstein JL, et al. Gastrointestinal toxicity with celecoxib vs nonsteroidal anti-inflammatory drugs for osteoarthritis and rheumatoid arthritis: the CLASS study: A randomized controlled trial. Celecoxib Long-term Arthritis Safety Study. JAMA 2000;284:1247-1255.
23. Arber N, DuBois RN. Nonsteroidal anti-inflammatory drugs and prevention of colorectal cancer. Curr Gastroenterol Rep 1999;1: 441-448.
24. Oshima M, Dinchuk JE, Kargman SL, et al. Suppression of intestinal polyposis in Apc delta716 knockout mice by inhibition of cyclooxygenase 2 (COX-2). Cell 1996;87:803-809.
25. Steinbach G, Lynch PM, Phillips RK, et al. The effect of celecoxib, a cyclooxygenase-2 inhibitor, in familial adenomatous polyposis. N Engl J Med 2000;342:1946-1952.
![]()
Home | Current Issue | Back Issues | Congress Calendar
Free Subscription | Editorial Board |