|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
From the Taipei International Breast Cancer Symposium, Introduction Dr King-Jen Chan opened the recent Taipei International Breast Cancer Symposium on behalf of the Breast Cancer Society of Taiwan and the MD Anderson Cancer Center in the USA. This important event provided a forum for internationally renowned scholars from the Asia-Pacific region and the USA to share their expertise in the diagnosis, treatment, and prevention of breast cancer as well as the basic science aspects of the disease. Welcoming the more than 400 delegates and speakers from 15 countries, Dr Chan expressed his hope that "the exchange of information [at this conference] will lead to further advances in the prevention and treatment of breast cancer as we enter the new millenium."
Alex Yuang-Chi Chang Since 1998, cancer has been the primary cause of death in Singapore (26%), closely followed by heart disease (25%), pneumonia (11%), and stroke (10%). Singapore has a comprehensive cancer registry, and every new case of cancer is registered. Breast cancer is the most common cancer among women in Singapore (figure 1), with an age- standardised rate of 46.1/100,000 women. This compares with a rate of 105/100,000 among white American women. Figure 1. Cancer incidence in Singapore.
The incidence of breast cancer in Singapore is increasing and is currently 5.7% per year among premenopausal women and 3.9% per year among postmenopausal women.1 The peak age is 45 to 49 years. Screening mammography is not routinely practised in Singapore, so this does not account for the increasing rate of breast cancer. However, possible explanations for the higher rate include the following: advanced medical knowledge, westernised diet and lifestyle, increased calorie intake, increased use of pesticides, radiation, and alcohol. The oestrogen receptor positivity rate in Singapore is lower than that in the USA (43% vs 60%). Breast cancer is most commonly diagnosed at stage II (table 1). BRCA-1 mutations are found in 8.6% of women with breast cancer aged less than 40 years and in 13.6% of women aged less than 35 years. 12.5% of women with a first degree relative with breast cancer have BRCA-1 mutations. The site of the mutation may differ from those in the West. Breast Cancer Screening There is no standard breast cancer screening programme in Singapore, although a national mammography trial that ran for 2 years from 1994 screened women aged 50 to 64 years. Only 42% of 67,656 women responded to an offer of free mammography and 97,294 women were enrolled as controls. These researchers were able to show that the disease could be diagnosed at an earlier stage with one screening mammogram (table 2).2 Table 1. Stage of breast cancer at presentation in Singapore
* p < 0.001
Treatment Treatment for breast cancer in Singapore is similar to that of western countries. For early disease, treatment generally takes the form of lumpectomy plus radiation therapy or mastectomy, sentinel node biopsy, or adjuvant chemotherapy and/or hormonal therapy. Interestingly, patients tend to favour mastectomy over lumpectomy. For locally advanced disease, neoadjuvant chemotherapy or mastectomy with radiation therapy will be offered, while there is a variety of treatment for metastatic disease, including hormonal therapy, chemotherapy, supportive therapy, radiation plus bisphosphonates, or biological therapy such as herceptin. The histology grade tends to be worse in the younger population, with 56% of women aged less than 40 years having poorly differentiated adenocarcinoma. Breast conservation tends to be higher for patients with stage I disease. The 5-year survival rate at the National University Hospital in Singapore is shown in table 3 the survival rates from the USA are shown for comparison. In Summary There has been a significant increase in the incidence of breast cancer in Singapore during the past 25 years. The peak incidence occurs at the age of 45 years, with most patients presenting with stage II or III disease. References 1. Seow A, Duffy SW, McGee MA, et al. Breast cancer in Singapore: trends in incidence 1968-1992. Int J Epidemiol 1996; 25:40-45. 2. Ng EH, Ng FC, Tan PH, et al. Results of intermediate measures from a population-based, randomized trial of mammographic screening prevalence and detection of breast carcinoma among Asian women: the Singapore Breast Screening Project. Cancer 1998; 82:1521-1528.
Louis Wing-Cheong Chow The incidence of breast cancer in Hong Kong is no different to that of Singapore or Taiwan. There has been an increase in incidence of breast cancer over the past 10 years, although the mortality rate has remained stable. Table 1 shows the incidence and mortality rates for 1995 to 1996. Table 1. Incidence of and mortality from breast cancer in Hong Kong during 1995 to 1996
Epidemiological studies into diet (calorie and cholesterol intake) found no difference in calorie intake between women with breast cancer and controls but the breast cancer patients had a slightly higher intake of cholesterol. Recently, more younger women are presenting with breast cancer, which could be due to increasing breast awareness and screening, although the reasons are un- clear. As in Singapore, there is no breast cancer screening programme in Hong Kong. T2 lesions (< 5 cm) are the most common staging at presentation, while locally advanced breast cancer is less frequent. Since 1995, more women have been presenting with early disease (< 2 cm). However, patients are presenting at a significantly younger age, particularly for T2-4 lesions. Since 1995, more patients have lymph node meta- stases than in previous years. Oestrogen receptor positivity diminishes with advancing stage, and is lower in the local population than in Caucasian women. Treatment in Hong Kong Data from Queen Mary Hospital on neoadjuvant chemotherapy for locally advanced disease (stages IIIA and B) show that the advantages of this approach to treatment include:
Several studies have shown that breast conservation after neoadjuvant therapy is possible. Figure 1. Tumour size before and after treatment with 5-fluorouracil, epirubicin, and cyclophosphamide (FEC) or adriamycin (A).
Contraindications for neoadjuvant therapy and breast conservation surgery include extensive residual disease or a multifocal tumour, positive resection margins, and non-compliant patients as well as a poor cosmetic outcome. Hong Kong Experience A retrospective analysis of 35 women with aggressive breast cancer was performed between March 1995 and December 1997. Patients were given either FEC (5-fluoruracil, epirubicin, cyclophosphamide) or adriamycin alone. The partial response rate was more than 60%, with a 13% complete response rate. The response rate was similar for both regimens used (figure 1), as was the mean survival rate. Interestingly, there was no correlation with survival and histological parameters in this group of patients, making it difficult to predict the response to treatment. However, biopsy of the primary tumour allows for design of treatment based on the response to chemosensitivity testing. In patients with locally advanced breast cancer, the choice of drug treatment based on histoculture drug response assay for neoadjuvant therapy gives a satisfactory tumour response and better prediction for breast conservation therapy.
Shin-Cheh Chen A study of 2658 patients with breast cancer without systemic metastases found that the incidence of breast cancer in Taiwan has increased from 14.52/100,000 in 1991 to 28.35/100,000 in 1996. The incidence is significantly increased in patients aged 40 to 49 years, with a median age of 47 years. While the proportion of patients younger than 35 years has decreased from 18.4% in 1990 to 9.2% in 1998, this is still much higher than in the USA (2.7%).1 The average size of the tumour at presentation has decreased from 3.5 cm in 1990 to 2.7 cm in 1998. The stages at presentation are shown in table 1. Histological type is not significantly different from that in the USA,2 with the exception of intraductal carcinoma, which has a lower incidence in Taiwan. There is a high percentage of diploid or tetraploid carcinoma (70%),3 but a lower percentage of oestrogen or progestrogen positivity (32%). Treatment The rate of partial mastectomy increased from 1.4% of patients in 1990 to 19.6% of patients in 1998. The relative survival and disease-free survival rates were similar to those for full mastectomy. The 9-year relative survival by TNM staging is shown in table 2 the data from the National Cancer Data Base in the USA is shown for comparison.4 Table 1. Tumour stage at presentation
The significant prognostic factors were stage, number of involved axillary nodes, age younger than 40 years, oestrogen receptor status, histological grade, and ploidy. The most frequent relapse sites were bone, chest wall, lung, liver, and neck. In Conclusion The incidence of and mortality from breast cancer in Taiwan is increasing, with evidence of geographic variation. The median age is younger than that of the West, with 10% of patients aged less than 35 years. Patients with early stage disease have a relatively good prognosis but the prognosis is not good in advanced disease. References 1. Bland KI, Menck HR, Scott-Conner CEH, et al. The National Cancer Data Base 10-year survey of breast carcinoma treatment at hospitals in the United States. Cancer 1998; 83:1262-1273. 2. Hunter CP, Epidemiology, stage at diagnosis, and tumor biopsy of breast carcinoma in multiracial and multiethnic populations. Cancer 2000; 88(Suppl.):1193-1202. 3. Shiao YH, Chen VW, Lehmann HP, et al. Patterns of DNA ploidy and S-phase fraction associated with breast cancer survival in blacks and whites. Clin Cancer Res 1997; 3:587-592. 4. Fremgen AM, Bland KI, McGinnis LS, et al. Cliical highlights from the National Cancer Data Base, 1999. CA Cancer J Clin 1999; 49:145-158.
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

 Breast Cancer Management in Singapore
Breast Cancer Management in Singapore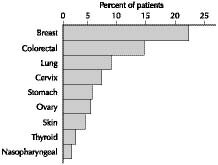
 Locally Advanced Breast Cancer in Hong Kong
Locally Advanced Breast Cancer in Hong Kong
 Characteristics of Breast Carcinoma in Taiwan
Characteristics of Breast Carcinoma in Taiwan
Home | Current Issue | Back Issues | Congress Calendar
Free Subscription | Editorial Board |