|
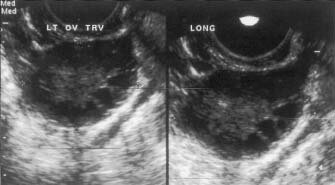
This ovarian ultrasound of a 30-year-old woman with PCOS shows characteristic multiple small 'cysts' in the ovarian cortex. PCOS is a relatively common condition, affecting up to 10% of women of reproductive age. It is the most common form of anovulatory infertility. Clinical features include menstrual disturbance secondary to this chronic anovulation or oligo-ovulation, and hirsutism or acne secondary to hyperandrogenaemia. Typically, as in this case, the patient presents with concerns about irregular menstrual periods and/or infertility, along with weight gain.
Diagnosis is based on the combination of ultrasound scanning of the ovaries using a vaginal probe and biochemical measurements1. Elevated free testosterone activity defined by the free androgen index is considered the most sensitive biochemical marker. A raised luteinising hormone (LH) concentration is also a useful indicator, but is now less favoured as a diagnositic tool.2
|
|
The pathogenesis of PCOS remains uncertain, but the link between this condition and insulin resistance is currently viewed as central, with resultant emerging therapies including the use of insulin-sensitising agents such as metformin.2
With regard to infertility, the most common therapeutic agent given is clomiphene citrate, generally taken daily from days 3-7 of the menstrual cycle. Intrauterine insemination is also frequently advised due to the adverse impact of clomiphene on cervical mucous quality.3.
References
1.Symonds EM, Symonds IM. Essential Obstetrics and Gynaecology. Churchill Livingstone 1998, 3rd ed.
2. Hopkinson ZEC, Sattar N, Fleming R, et al. Polycystic ovarian syndrome: the metabolic syndrome comes to gynaecology BMJ 1998;317:329-332.
3. Bay Area Fertility & Gynecology Medical Group Polycystic Ovary Syndrome (PCOS) http://www.ccnet.com/bafertil/pcos.html
|