|
|

|
|
|
|
|
The Swollen Optic Disc: Further Observations of a European Neuro-Ophthalmologist in Southeast Asia JF Cullen With the increased incidence of brain tumours in Southeast Asia and the common complaint of headaches among patients attending eye departments, clinicians should be concerned that they may miss such conditions, which tend to present and be diagnosed at a late stage in Asia. The swollen disc of papilloedema is, along with headache, the characteristic manifestation of raised intra-cranial pressure commonly associated with a brain tumour. It should be reassuring therefore for the examiner to be able to determine whether a suspicious optic disc is within normal limits or not.
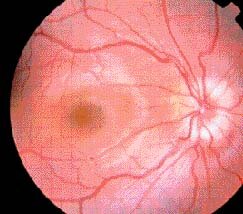
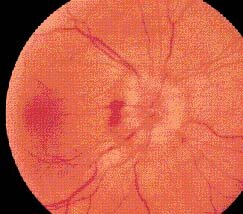
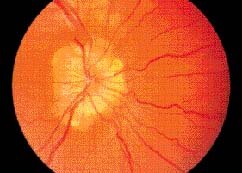
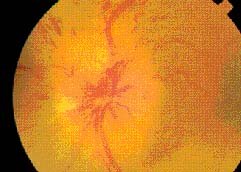
Papilloedema The term papilloedema is now accepted as describing that specific form of optic disc oedema (Figure 1) associated with raised intracranial pressure. Papilloedema is easily diagnosed in its established state when it is bilateral and haemorrhages and or exudates are evident on the disc itself or at the margins (Figure 2). Visual acuity is normal and field testing may only demonstrate an enlarged blind spot. Peripheral constriction of the visual field is a late finding which may be associated with post-papilloedema optic atrophy.1 In the early stages, papilloedema may be difficult to distinguish from variants of normal (pseudo-papilloedema) but the latter does not change over a period of observation and, when in doubt, re-examination after 2 to 3 weeks is required. Contrary to traditional teaching, the first areas of the disc to become blurred or elevated are the lower and upper margins rather than the nasal side; in cases of uncertainty these areas should receive special attention. Not all patients with papilloedema harbour a brain tumour. Raised intracranial pressure can be associated with hydrocephalus, especially in children, or can follow a head injury. It is also found in pseudo tumour cerebri (benign intracranial hypertension; BIH), which generally occurs in young overweight females. Referral to a neurosurgeon is not required until the ophthalmologist has confirmed the diagnosis and carried out a computerised tomography (CT) or magnetic resonance imaging (MRI) scan.
When papilloedema is present or suspected, other ocular abnormalities should be looked for such as nystagmus, pointing to a lesion in the posterior fossa, and a sixth nerve palsy may be a false localising sign. A homonymous field defect can indicate compression of the supra-geniculate or posterior visual pathway by a tumour such as a glioma, meningioma, or an arterio-venous malformation. The headaches of raised intracranial pressure are usually worst in the mornings, centred in the frontal region, and are aggravated by bending down.
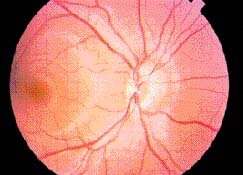
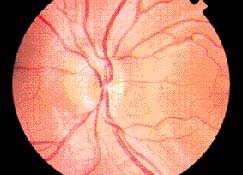
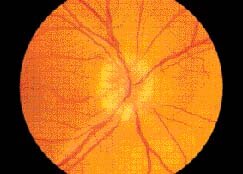
Pseudopapilloedema, also termed pseudo-neuritis or pseudopapillitis, is the commonest cause of a mistaken diagnosis of true papilloedema (Figure 3). Figure 3 shows the discs of a 12-year-old boy who was referred with a diagnosis of papilloedema and brain tumour based on his disc appearances and a mistakenly interpreted brain scan. Pseudopapilloedema is usually associated with refractive errors of hypermetropia and/or astigmatism or tilted discs, as in this patient. The disc margins are blurred and the disc itself may appear elevated. The cup is often absent but there is no true oedema and the veins are of normal calibre and pulsate normally. It is usually bilateral and symmetrical and does not change over a period of observation. If in doubt, fluorescence angiography (FFA) distinguishes it from papilloedema or optic neuritis (papillitis) by the absence of dye leakage, especially in the late stages of the passage of dye through the retinal vessels. Other conditions less likely to give rise to a misdiagnosis of papilloedema are opaque nerve fibres (Figure 4), congenital fibrous tissue overlying the disc, and, more importantly, optic nerve head drusen (Figure 5), also termed hyaline bodies of the optic disc where the nerve head is elevated and, as in Figure 5, hyaline deposits may be multiple and extend out beyond the disc margins, and an abnormal branching of the retinal vessels is also commonly present.
In this condition the nerve head is usually small a so called 'crowded disc' and the anomaly is generally bilateral and sometimes familial. However, when the hyaline material is buried within the disc substance, diagnosis will be difficult, especially if a field defect is also present.
Optic Neuritis Acute inflammation or demyelination of the optic nerve (optic neuritis or papillitis) usually presents in young patients with sudden unilateral loss of central vision, a relative afferent pupil defect, and a swollen hyperaemic disc (Figure 6). In Europe, this is the less common manifestation of optic neuritis (about 35% of cases), or of what is more correctly termed anterior optic neuropathy, as opposed to retrobulbar optic neuropathy (65%). In Southeast Asia, however, a swollen disc (papillitis) is the more common manifestation of optic neuropathy, occurring in two-thirds of patients and multiple sclerosis is a rare cause in this region. Spontaneous recovery is still the expected outcome and corticosteroid treatment is still controversial. According to Walsh and Hoyt, MRI scanning is not required to establish the diagnosis of optic neuritis.2
Other Causes of Optic Disc Oedema Hypertensive Retinopathy and Other Retinal Vascular Diseases In hypertensive retinopathy, central vein occlusion, and other retinal vascular diseases, the disc may be swollen with haemorrhages and/or exudates. However, the latter are not confined to the immediate disc area as in the conditions described above, and other evidence of vascular disease or abnormality is usually clearly evident in the mid and peripheral fundus.
Anterior Ischaemic Optic Neuropathy Anterior ischaemic optic neuropathy (AION), both arteritic due to giant cell arteritis and the non-arteritic variety (NAION) usually associated with diabetes, hypertension or arteriosclerosis, present in elderly people with sudden severe visual loss or blindness in 1 eye which may become bilateral if not treated or prevented.
Figure 10. Computed tomography scan showing right optic nerve sheath meningioma note thickened nerve.
|
|
Address for correspondence
JF Cullen, MD, FRCS, FRCSE |
![]()
![]()
Home - Table of Contents - Current Issue - Back Issues -
Congress Calendar - Editorial Board - - Free Subscription