|
Manual Small Incision Sutureless Modified Phaco-sandwich Technique Using Singh Vectis
G Singh,1 J Kaur2 1 Regional Eye Institute, 2 Hi Tech Eye Care and Laser Centre, E1/ 114, Arera Colony,
Bhopal, India
Introduction

The two main objectives of modern cataract surgery are to minimise surgically-induced astigmatism and to achieve rapid visual rehabilitation. Clear corneal or scleral tunnel incisions of the minimum possible size are the key to achieving these objectives. Today, phacoemulsification has surpassed multiple large incision extra capsular cataract extraction as the method of choice among most surgeons in developed countries. The advantages of phacoemulsification are that it gives excellent post-operative astigmatic control, early visual recovery, and better wound stability, especially in the early postoperative period. Although phacoemulsification has become the biggest surgical achievement of the present decade, it is still not being practised by the majority of surgeons in developing countries such as India. Two important reasons for this are that the technique has a prolonged and sometimes traumatic learning curve and, secondly, it requires expensive and complex equipment. Manual small incision sutureless cataract surgery using various methods is thus a good and effective alternative in this situation. The technique of manual sutureless phaco-surgery offers the following advantages:
- it preserves the integrity of the limbal anatomy thus minimising post-operative astigmatism
- there is early wound stabilisation (after approximately 2 weeks)
- no sutures are used, thus all suture-induced problems are eliminated
- it is safe and easy for mature and hyper-mature cataracts
- it is cost effective (both initially and for maintenance)
- it is less likely to cause complications such as posterior capsule rupture, dropped nucleus, and bullous keratopathy
- it can even be performed for hard nuclei or incomplete continuous circular capsulorhexis
- it is a good alternative for eye camp surgery.
Surgical Technique
In general, there are 2 methods for performing manual small incision sutureless extracapsular cataract extraction, namely:
- extraction of the nucleus after fragmentation
- extraction of the nucleus as a mass without fragmentation.
In the first method, the incision size is relatively smaller (between 3.5 and 5.5 mm) than in the second, which varies from 6.0 to 8.0 mm. When fragmentation of the nucleus is done, the technique basically involves the 2 stages of fragmentation of the nucleus and extraction of the fragmented pieces of nucleus. Among the medium incision techniques (5.5 to 8.0 mm) are the techniques of nucleus suction with a Simcoe cannula, as modified by Beirouty et al.,1 Fry's phaco-sandwich technique,2 and those based on reducing the size of the nucleus such as the Blumenthal Mini Nuc technique.3 Small incision techniques (3.5 to 5.5 mm) include Kansas Bisection and Trisection,4 Keener's stainless steel loop techniques,5 Quintana's 3-0 nylon loop technique,6 and Gutierrez' technique using his specially designed nucleotome.7
Personal Opinion
We have tried almost all of the above-mentioned techniques and feel that, in India, where the majority of patients report late for surgery and when the size of the nucleus is relatively large, any technique which involves multiple manipulations for fragmenting the nucleus and later removing the broken fragments, makes the surgery more difficult with an increased chance of trauma to both the uveal and corneal tissue. It further increases the dependence on better quality viscoelastic material, which, unfortunately, increases the cost of surgery for patients, thereby defeating the main purpose of using cost-effective manual non-phacoemulsification procedures.
Modified Phaco-sandwich Technique Using Singh Vectis
We have used the modified phaco-sandwich technique for the past 3 years with satisfactory results for more than 500 patients with cataract. In this technique, the nucleus is removed en mass through a 6 to 7 mm scleral tunnel incision using a self-designed lens vectis (Ankur Metal Works, Calcutta, India) and standard Sinsky's hook. The main advantage of this technique is that there is minimum manipulation of the nucleus in the anterior chamber, so chances of possible trauma to both iris and corneal endothelium are minimised. The only disadvantage is that a relatively large incision is required, depending on the size of the nucleus and it is slightly difficult for beginners to dissect a relatively large self-sealing scleral tunnel. Also, since the tunnel length is longer, the shift in postoperative astigmatism is from 1.0 to 1.25 diopters for the majority of patients.
Singh Vectis
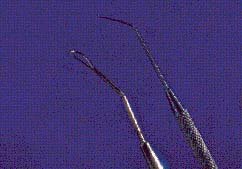
We use a lens vectis (Figure 1) that we have modified from Akura's claw vectis.8 It has an initial loop, the tip of which is slightly curved to give a good grip to the nucleus during extraction. In addition, there are 2 more angulations designed in such a way that, during the bimanual insertion of the vectis and Sinsky hook, there is a minimum chance of touching and damaging iris tissue and the posterior capsule below and corneal endothelium above.
Figure 1. Singh vectis and sinsky hook
Surgical Technique
After peribulbar block, a fornix-based conjunctival flap is made. All episcleral vessels are cauterised using bipolar cautery. A frown-shaped scleral incision is made using a standard number 15 disposable blade. The width of the tunnel is redetermined by the size of the central nucleus, which is assessed by slit-lamp before surgery; between 6 and 7 mm for the majority of patients. A crescent knife is then used to dissect the scleral pocket. The ends of the frown incision are approximately 3.0 mm from the limbus while the central convexity is approximately 1.5 mm from the limbus. The tunnel is extended by about 2.0 mm into clear corneal tissue. A 3.2 mm angled keratome is then inserted into the scleral pocket and entered into the anterior chamber. While the keratome is entering the anterior chamber, the internal lip of the wound is clearly seen. The anterior chamber is then filled with 2% methylcellulose.
A relatively large circular capsulorhexis (6.0 to 6.5 mm) is then made using the bent tip of a 26 G needle. A can-opener technique may be required for a large nucleus. For patients in whom a central circular capsulorhexis is done, 2 relaxing incisions are vertically made for easy prolapse of the nucleus without undue pressure on the zonules. Then using the Blumenthal hydro-dissection cannula, hydro procedures are performed until the hard central nucleus core is isolated.2 Simultaneously, with the tip of the same cannula, the nucleus is rotated and manually lifted from the superior pole. This simultaneous rotation and lift movement is continued until the nucleus is totally prolapsed in the anterior chamber. This is the most important step in the technique since all manipulations are done in a closed chamber. Viscoelastic is again injected over the prolapsed nucleus to deepen the anterior chamber and a side-port entry is made at 2 o'clock using a V-lance knife.
The scleral tunnel is then enlarged to its full length. Viscoelastic is again injected above as well as below the prolapsed nuclear mass and the posterior capsule with the posterior epinucleus is pushed back as far as possible. Thus, a good cushion of viscoelastic is made both in front and behind the nucleus. Then, with a bimanual technique, the Singh vectis and Sinsky hook are entered simultaneously under clear vision and the nuclear mass is sandwiched between the 2 instruments. With gentle pressure, the nucleus is prolapsed out of the scleral pocket incision.
The epinucleus is then hydro-expressed using the Simcoe cannula with simultaneous gentle pressure at the scleral incision, thus creating a fish mouthing phenomenon. This procedure expresses the epinucleus in a circular manner. Care must be taken not to apply excessive pressure on the wound at this time. The residual cortex is then removed using the Simcoe bi-way cannula. A 6 mm polymethyl methacrylate (PMMA) intraocular lens (IOL) is then inserted after inflating the bag with viscoelastic. The lens is "dialled" into position using the Sinsky hook and all residual viscoelastic is aspirated out. Irrigating fluid is injected from the side port incision to close the internal lip of the tunnel. The conjunctiva is then replaced over the wound and cauterised at the 2 ends using co-optation forceps.
Exclusion criteria for this technique include:
- hard cataracts (grade V)
- maximum pupillary dilatation less than 6 mm
- relatively shallow anterior chamber
- pre-existing ocular disorders such as uveitis, glaucoma, or subluxation.
Clinical Trial
We studied 300 eyes of 275 patients (62% male, 38% female) with a mean age of 58.5 years (range, 38 to 80 years) who underwent modified phaco-sandwich sutureless surgery from 1 January 1999 to 1 October 2000. All surgeries were performed by the same surgeon using the above-mentioned technique. Nucleus hardness was graded using Emery and Little's classification.9 Grade distribution was as follows:
- grade 1 30 eyes
- grade 2 186 eyes
- grade 3 76 eyes
- grade 4 8 eyes.
Mean follow up was 8 months (range, 2 to 22 months). The mean incision width was 6.1 mm (range, 6.0 to 8.0 mm). In 10 eyes, the wound was larger than 7.5 mm. Sutures were not required for any patients. The nucleus was bisected in 36 eyes during extraction of the nucleus in this situation each segment was removed using the same technique. Intraoperatively, 6 eyes had a posterior capsular rent. In 2 eyes, the rent occurred during the insertion of the lens vectis as there was sudden shallowing of the anterior chamber. In the remaining 4 eyes, the rent occurred during the cortical clean up. In 4 eyes, repeated iris prolapse occurred due to premature entry to the wound in these cases a higher grade of viscoelastic (Healon) was used to prevent iris trauma.
The most common complication was transient striate keratopathy, which was seen in 24% of eyes. This did not persist for longer than the first postoperative week. In 28% of patients, a can-opener capsulectomy was done, either due to a non-dilating pupil or where the capsulorhexis was eccentric. In one patient, iridodialysis occurred due to inadvertent catching of iris tissue with the tip of the Sinsky hook.
A transient rise in intraocular pressure occurred in 4 eyes, which were all controlled with medical therapy. Intraocular lens implantation was not deferred for any patients. Mean surgically-induced astigmatism (the change in the corneal curvature determined by the difference between the pre- and postoperative keratometry) was found to be 1.62 D (range, 1.0 to 2.5 D) at the end of the fourteenth postoperative day. This was calculated using the Jaffe and Clayman vector analysis.10
Best corrected visual acuity (BCVA) of 6\12 or better was achieved at the end of the second postoperative week for 92% of patients. For those patients where it was less than the baseline, the cause was not related to the surgical procedure there was age-related macular degeneration of different grades in 18 eyes, while in the remaining 6 eyes there was optic disc pallor.
We compared these results with a series of phacoemulsification procedures using a 5.25 mm incision (PMMA IOL) and a 3.5 mm incision using a foldable IOL. Statistical analysis showed that the change in astigmatism induced surgically ranged from 1.0 to 2.0 D for more than 80% of patients for whom the manual phaco-sandwich technique was performed, while for those patients in whom the 5.25 mm PMMA IOL was used surgically-induced astigmatism ranged from 0.75 to 1.25 D in an equal percentage of cases. Among patients receiving a foldable IOL, the range was 0.6 to 1.0 D.
Discussion
Both phacoemulsification and manual phaco-sandwich techniques are used at our institution. We consider both the techniques to be equally useful, especially when not using a foldable IOL.
Our experience has shown that, just as in phacoemulsification where adequate pupillary dilatation and good endothelial count with adequate anterior chamber depth are essential prerequisites for achieving successful surgery, so is the case for manual small incision sutureless phaco-sandwich surgery. The final visual outcome has been encouraging with a minimum of vision threatening complications with our technique and we have found that this technique is a good alternative to phacoemulsification surgery. It enjoys all the advantages of modern phacosurgery and also serves as an intermediate step for those surgeons who wish to convert to the phacoemulsification technique.
Recently, we have tried this technique with topical (preservative free) 1% lignocaine alone and with topical plus intracameral (preservative free) 1% lignocaine. The results have been equally encouraging and we now regularly perform this surgery using only topical anaesthesia for cooperative patients with good preoperative conditions.
References
1. Beirouty Z, Barker NH, Shanmugam SN. Sutureless one-handed small incision cataract surgery by manual nucleosuction a new technique for cataract extraction. Eur J Implant Refract Surg 1995;7;295-298.
2. Fry LL. The phacosandwich technique. In: Rozakis GW, editor. Cataract surgery: alternative small-incision techniques. Thorofare, NJ: Slack; 1990; 71-110.
3. Blumenthal M. Manual ECCE, the present state of the art. Kin Monatsbi Augenheikd 1994;205:266-270.
4. Kansas P. Phacofracture. In: Rozakis GW, editor. Cataract surgery: alternative small-incision techniques. Thorofare, NJ: Slack; 1990;45-69.
5. Keener GT Jr. The nucleus division technique for small incision cataract extraction In: Rozakis GW, editor. Cataract surgery: alternative small-incision technique. Thorofare, NJ: Slack; 1990:163-191.
6. Quintana M. Implantacion de LIO plegable con facoseccion manual y pequena incision. Microcirugia Ocular 1998;6(1):37-44.
7. Gutierrez FJ. Manual multi-phaco fragmentation through a 3.2 mm clear corneal incision. J Cataract Refract Surg 2000;26:1523-1528.
8. Akura J, Kaneda S, Hatta S, Matsuura K. Manual sutureless cataract surgery using a claw vectis. J Cataract Refract Surg 2000;26:491-496.
9. Emery JM, Little JH. Phacoemulsifi-cation and aspiration of cataracts: surgical techniques, complications and results. St. Louis, MO CV Mosby; 1979: 45-48.
10. Jaffe NS, Clayman HM. The pathophysiology of corneal astigmatism after cataract extraction. Trans Am Acad Opthalmol Otolaryngol 1975;79: 615-630.
|
Address for correspondence
Dr Jagmeet Kaur
Hi Tech Eye Care & Laser Centre
E -1/114, Arera Colony
Bhopal
India, 462016
E-mail:
|
|
Set the Agenda for Your Journal
As practising ophthalmologists in the Asia-Pacific region, Asian Journal of OPHTHALMOLOGY is your Journal. Asian Journal of OPHTHALMOLOGY is intended to be a vehicle for the exchange of information relevant to clinical practice in Asia. Make the Journal work for you by sending your letters, contributions, articles, meeting reports and announcements, and any other information that may interest your colleagues. By telling us what you would like to see published in Asian Journal of OPHTHALMOLOGY, you can make this truly your Journal.
Please send your contributions to:
|
The Editor
Asian Journal of OPHTHALMOLOGY
Scientific Communications (Hong Kong) Ltd
4/F, 11 Queen Victoria Street
Hong Kong
|
|
Tel:
Central Fax:
E-mail:
|
|
 
|
